
Abortion and Mental Health: A Review
Abortion and Mental Health: A Review
Getting an abortion is not causally related to low mental health.

In a previous post of mine, I discussed the research surrounding the relationship between abortion and psychological well-being (see Black 2022). However, the article was about multiple things related to abortion and not primarily on mental health. In contrast, this article seeks to review the literature on the effects of getting an abortion on mental health and being denied an abortion.
To summarize, I will argue that there is no causal relationship between receiving an abortion and low mental health. Furthermore, being denied an abortion affects one’s mental health, for various reasons. Please consider buying a subscription to the Substack, or even subscribing for free, (being a paid member is way better), and share this article.
Abortion and Mental Health
In one of the most commonly cited studies 1, Coleman (2011) found that women who have had an abortion had an 81% increased risk of mental health issues, according to data ranging from 22 studies published between 1995 and 2009. According to Coleman, 10% of the variance could be attributed to the abortion itself, leaving the rest unexplained.

Despite the positive citation of Coleman by many pro-life websites, there are significant issues with Coleman’s meta-analysis, which still seems to be cited in government hearings when discussing the issue of abortion.2 Steinberg et al. (2022) identified a number of critical errors in Coleman's meta-analysis. The first notable misstep was Coleman's failure to adhere to established guidelines for conducting a meta-analysis. Coleman did not provide adequate details regarding his inclusion criteria, and alarmingly, a substantial portion of the papers included in his analysis, specifically 11 out of 22, were authored by Coleman himself. This apparent conflict of interest raises concerns about the objectivity of the analysis.
The second significant error was Coleman's treatment of effect sizes as independent entities rather than dependent variables. Given that there were 14 distinct data sets involved in the study, it was imperative to analyze 14 effect sizes. However, Coleman reported a total of 36 effect sizes, indicating a fundamental methodological flaw. Additionally, Coleman's calculation of the population-attributable risk was problematic. He concluded that 10% of the variance could be attributed to mental health, but it's essential to note that a population-attributable risk can only be accurately calculated when causation is definitively demonstrated. Thus, Coleman's use of variance data in this context was not appropriate and introduced further uncertainty into his analysis. Furthermore, Coleman's study exhibited several additional errors, such as deviations from his own inclusion/exclusion criteria, misclassification of comparison groups, inappropriate adjustments of effect sizes for various factors that were not uniform across the studies, and the drawing of invalid inferences. Moreover, the quality of many of the studies cited by Coleman was subpar, lacking appropriate controls, which raises questions about the validity of the findings derived from his study.
Abel (2012) provides further issues with Coleman’s analysis. Specifically, Coleman failed to follow a methodology common to systemic reviews, with no information given on how the studies included in the original Coleman analysis were chosen to be included due to the lack of criteria information. As Abel notes, “This is particularly important here as many of the primary studies included in this review have significant methodological limitations, including non-prospective design, non-standardised measures of mental disorders, lack of adjustment for pre-existing mental illness, lack of adjustment for other key confounders (e.g. social deprivation), non-comparability of exposed and non-exposed groups, and selection bias” (74). Further issues have been noted about the Coleman analysis in other academic works (Kendall et al., 2012; Littell and Coyne, 2012; Puccetti et al., 2012; Lagro-Janssen et al., 2012; Robinson et al., 2012), mainly repeating the issues noted in Abel and Steinberg et al.
Akin to the Coleman analysis, Reardon and Cougle (2002) and Reardon, Cougle, and Coleman (2003) found that getting an abortion was associated with associated with depression, according to data from the NLSY. The results held in the Reardon, Cougle, and Coleman analysis after controlling for age, race, marital status, divorce history, education, income, and external locus of control scores.

In a critical comment on Reardon and Cougle from Schmiege and Russo (2005), they note issues with their coding. There was a misidentification of unwanted first pregnancies and exclusion of women with a high risk of depression associated with early childbirth. Once the same analysis with proper coding was conducted, there were no significant differences in depression rates between women who had abortions and those who did not.

In response to Reardon and Cougle (2002), Major et al. (2009) remark significant issues with this analysis. First, the re-analysis by Schmiege and Russo also makes note of the miscoding errors present in Reardon and Cougle’s work. Second, the I-E scores, which were used to adjust for prior mental health, did not actually measure mental health. The restriction of range in the sample also excluded 339 of 425 of the teenagers who did not take the I-E measurement. Finally, people with certain scores were cut out of the analysis, and multiple people of different races were included in the “white” category, despite not being white (40). Despite these issues, Reardon and Cougle’s work is still cited in a positive manner by critics of abortion. 3
Pederson (2008) used a nationally representative sample and found a positive relationship between getting an abortion and depression (aOR = 2.9). It’s no surprise to see that, much like the other studies, the Pederson data has also been cited positively by anti-abortion critics. 4 A look at the regression shows that the abstract is a bit misleading, though (see Black, 2022 for more information on the issue of misleading information on abstracts).
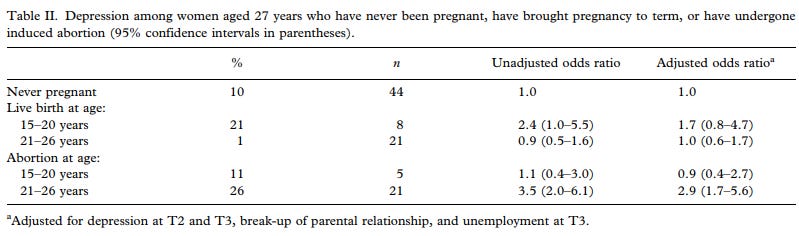
As can be seen, the relationship only exists for those between the ages of 21 to 26. For those 15-20, the odds ratio indicated a decrease and not an increase. The relationship indicated an increase in the odds for those aged 21-26, but the small sample is an issue in the study. It’s unknown how rigorous the controls were as it was only depression at T2 and T3, break-up of parental relationship, and unemployment at T3 (T = time, longitudinal data).
Sullins (2016) found similar results to Pederson and seems to have more controls than the prior analysis. Much like Pederson, there was a relationship between getting an abortion and mental health issues, after adjusting for prior-mental health, age, race, parental education, childhood poverty, and region of origin.

Contrary results were found in Warren, Harvey, and Henderson (2010), who also used the same data set as Sullins but only focused on 5 years. For depression, there was no relationship, with age, race/ ethnicity, living with parents, and family economics. Abortion was not associated with depression in waves 2 or 3.

In the case of self-esteem, similar results were found. Abortion did not predict low self-esteem in other waves. For both analyses, only prior depression and low self-esteem predicted depression and low self-esteem.

Fergusson, Horwood, and Boden (2008) utilized longitudinal data of more than 500 women from New Zealand. Variables like childhood socioeconomic status, parental adjustment, family functioning, exposure to child abuse, individual characteristics, and achievement, adolescent adjustment, and lifestyle were used as covariates. They found a relationship between getting an abortion and low psychological well-being.

There are a few issues with this analysis though. First off, some of the CIs in the study are wide, especially in the 5-year lagged model which is based on a longitudinal data set. Second off, as the Gutmatcher Insistute notes:
The 2008 Fergusson study likewise did not separate women who had multiple abortions from those who had only one, and it did not account for underreporting of abortion. This study also did not determine that women who had abortions were more likely than women who had unintended births (or other pregnancy outcomes) to have subsequent mental health problems; instead, the authors compared women who experienced each pregnancy outcome (abortion, pregnancy loss, unintended birth, intended birth) with women who had not experienced that particular pregnancy outcome (e.g., women who had an abortion were compared with all women who had not had an abortion, when the appropriate comparison group would have been all other women whose unintended pregnancy did not end in abortion).
Fergusson, Horwood, Boden (2013) conducted a meta-analysis and found that “There is suggestive evidence that abortion may be associated with small to moderate increases in risks of some mental health problems.” However, some of the studies used to come from Coleman’s paper cited above, so there’s no reason to take this analysis seriously. The question of causality is also not supported, as based on the evidence cited above and below.
Gissler, Hemminki, and Lonnqvist (1996) looked at 9, 192 women who had an abortion and gathered data from some of their birth certificates, specifically because they used nationwide data from Finland. Women who had abortions were more likely to commit suicide at all age levels than the reference group.

As the APA Task Force found (see Major et al. or click here for full review), the 1996 study failed to adjust wantedness, exposure to violence, class, and parity. The group comparisons were, thus, problematic, and the small sample size across cohorts is another issue. The issue of abortion and the risk of suicide has been noted in other analyses (e.g., Zheng, Yang, and Zhen, 2020).
However, the temporal relationship is unknown. Does getting an abortion increase the risk of suicide, or is the risk of suicide present prior to an abortion? In Steinberg et al. (2019), the researchers made use of Danish registry data spanning from 1980 to 1998. It was found that while there was an increased risk of suicide post-abortion when compared to women who did not get an abortion, that risk was also there a year before the abortion.

This risk decreased as time went on from 1-5 years (aIRR = 1.90) and 5 years more or later (aIRR = 1.73). Similarly, Steinberg, Becker, and Henderson (2011) found that once further variables were adjusted, abortion was not related to depression, suicide ideation, and self-esteem.

Taken together, these findings display that getting an abortion is not related to the risk of suicide, specifically because the risk is there before one gets an abortion and because getting an abortion is not related to suicide ideation.
It should be no surprise that the same effects, or lack thereof, are also found when looking at abortion and mental health, too. In a comprehensive study conducted by Steinberg, McCulloch, and Adler (2014), involving a sample of 259 women who had undergone abortion and 677 women who had experienced childbirth, rigorous statistical adjustments were applied. These adjustments accounted for several crucial factors, including the presence of pre-existing mental health issues before the first abortion or childbirth, pre-pregnancy exposure to adverse circumstances, a history of pre-pregnancy miscarriages, age at the time of the first pregnancy, racial or ethnic background, and the economic status experienced during childhood.

Upon meticulous statistical scrutiny, the study revealed that abortion did not emerge as a statistically significant predictor of various mental health outcomes. Specifically, abortion was not found to be associated with heightened levels of anxiety, mood disorders, impulse control issues, eating disorders, or suicidal ideation, after accounting for the aforementioned covariates.
Much like their prior meta-analysis, Coleman et al. (2009) found that abortion had adverse effects on psychological well-being, while also calculating a population-attributable risk. However, as was already noted in the issues with Coleman’s meta-analysis, we can not calculate a population-attributable risk if the relationship is not causal. Indeed, contra Coleman et al., Steinberg and Finer (2012) note how they were unable to replicate the Coleman et al. analysis in their analysis (Steinberg and Finer, 2011). when prior mental health and violence experiences were adjusted, there was no relationship between having had an abortion and anxiety disorders.
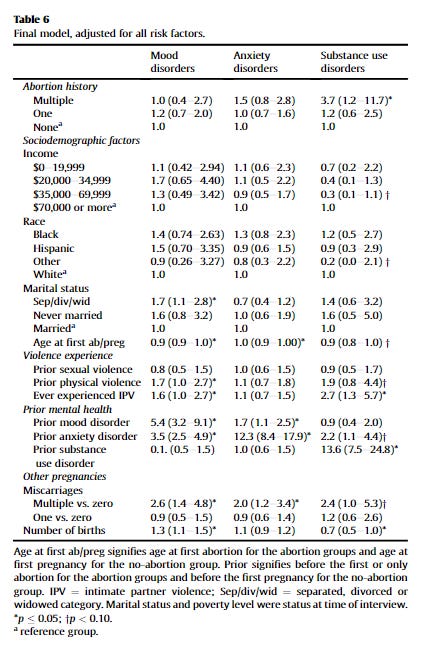
As Steinberg and Finer note, Coleman et al. did not use the correct weights in their analysis. In their updated regression, they made false claims about their dependent variables and their findings. Coleman et al. “not only use inappropriate measures of psychiatric diagnoses, but repeatedly claim that they are using something else” (1). They claim to use one measurement, but in reality use another, like saying they used a 30-day diagnosis and then a 12-month measurement. Their replication regression only supported their original findings because they didn’t use the 12-month measurement for mental health or the 30-day one, but rather lifetime.
As is said, the utilization of lifetime diagnoses in the research, which may create the impression of 30-day diagnoses to the readers, significantly undermines the meaningfulness of the findings and fails to support several statements that persist within the paper. A particularly notable example can be observed in Table 6, which presents measures of population attributable risk. The validity of these measures is questionable because there is no way to ascertain definitively that the abortion occurred prior to the onset of the mental health problems.
In their original discussion, which remains unaltered in the corrigendum, Coleman et al. make comments that presuppose a temporal sequence wherein abortions preceded the diagnoses of mental health issues. For instance, they refer to "post-abortion mental health problems" (p. 775), assert that their study "is essential to the process of clarifying the mental health risks unique to abortion" (p. 776), and express the need for future research to investigate the mediating mechanisms linking abortion to various disorders. It's important to acknowledge that these statements and analyses are fundamentally flawed given that the mental health diagnoses employed were based on lifetime assessments. Once again, despite the bad data, Coleman et al. continue to be cited. 5 Readers interested in the issues with Coleman’s analysis are referred to footnote 6. 6
Steinberg and Russo (2008) conducted a comprehensive investigation that considered a multitude of factors to better understand the association between first-pregnancy outcomes and subsequent anxiety. Their analysis accounted for a range of variables, including pre-pregnancy anxiety symptoms, a history of rape, the age at which the first pregnancy outcome occurred (abortion versus delivery), race, marital status, income, educational attainment, subsequent abortions, and subsequent deliveries.

For women who had experienced only one abortion, Steinberg and Russo's findings did not reveal any significant relationship between the initial pregnancy outcome and the development of generalized anxiety disorder, social anxiety, or post-traumatic stress disorder. However, when examining women with multiple abortions, a noteworthy relationship emerged between the initial pregnancy outcome and subsequent social anxiety and post-traumatic stress disorder. Importantly, this relationship was substantially explained by pre-existing mental health disorders and exposure to violence. Similar results were again found in Foster et al. (2015).
Holmlund et al. (2020) found that having an abortion was not associated with one’s psychological well-being or parental efficacy.

Based on the best available evidence, there does not seem to be a relationship between getting an abortion and low mental health post-abortion. The relationship is not causal, as psychological issues seem to come before one gets an abortion, and adjusting for covariates shows no differences between those who do and do not get an abortion. Studies finding a negative effect have been criticized for their methodologies (see Major et al.; National Academy of Science). Indeed, these were the findings of Major et al. and Charles et al. (2008), who found that the highest-quality studies were more likely to find no effect or were neutral, but studies with flawed methodology were more likely to find negative effects.
The same issue follows abortion and substance abuse. As Pederson (2007) found, women who had an abortion were more likely to abuse substances. As was noted above with the issue of the temporal relationship between abortion and mental health, substance abuse comes before one gets an abortion — also showing no causal effect. Roberts et al. (2018) found that women who had abortions and abused drugs and alcohol did so before they even knew they were pregnant. Many of the substances use either decrease as time goes on are stays linear.

Based on this evidence, there is no causal relationship between getting an abortion and adverse psychological effects. Of the studies with better methodologies, they fail to find a relationship — despite the studies finding a relationship continuing to be cited by pro-life organizations and being cited in congressional hearings.
Future research should examine the issue of moral incongruence on the effects of abortion. Even if the relationship is not causal, there might be an indirect effect where views on abortion might impact well-being if one gets an abortion. If one gets an abortion, despite being against abortion, it could cause adverse effects because going against one’s own morals — but not getting the abortion itself, per se — causes adverse effects. As is shown in the literature on pornography (see link below),

watching pornography is not causally associated with adverse effects. Rather, going against one’s own morals (i.e., watching pornography despite being morally against it) is what causes adverse effects. As far as I am aware, only one study (Conklin and O’Connor, 1995) on abortion and views on a fetus has found support for the moral incongruence model, though it was not described as such but may still follow the same general mechanism.
Denied an Abortion and Well-Being
After the contemporary ban on abortion among some U.S. states, the question of if being denied an abortion might impact psychological well-being is of current importance. Of the studies that have been conducted on those who have been denied an abortion, we find that those who are denied an abortion experience low psychological well-being.
Looking at a longitudinal data set of 956 women, those who were denied an abortion experienced lower self-esteem, anxiety symptoms, life satisfaction, but similar depression levels to those who got an abortion. These effects decreased as time went on or remained constant (Briggs et al., 2017).

Rocca et al. (2013) remarked that women who were denied an abortion experienced more anger and regret, and less relief and happiness. Interestingly enough, most women who got an abortion (95%) and those who expressed regret (89%) felt that getting an abortion was the right decision.

Rocca et al. (2021) found that after a week of being denied an abortion, there were both positive and negative emotions. Emotions became less negative and more positive as time went on, with lower social support, more difficulty deciding to seek abortion, and placing the baby for adoption being associated with reporting more negative emotions. Similarly, those denied an abortion did not see a change in drug use, frequency of drug use, and cannabis use over time. However, those who were denied an abortion and ultimately gave birth did increase their drug use, besides cannabis, when compared to those in the Near Limit Abortion Group, who did not increase use (Roberts, Rocca, and Foster, 2014).

For well-being, the effects seem to be complicated; for substance abuse, the effects also differ. Being denied an abortion, though, does seem to impact other areas that might affect one’s well-being. As was discussed by Foster et al. (2018) women who are denied an abortion are more likely to experience economic hardship and insecurity in the following years. It can also affect relationship quality, as noted by Upadhyay et al. (2022), who found that women denied an abortion were more likely to be in a poor relationship, quality-wise.

In conclusion, being denied an abortion does seem to have adverse effects. It can affect psychological well-being, and relationship quality, but depends on substance abuse.
See, e.g., Life Insitute, n.d., Taylor 2018; Shuping and Shaler, n.d., from the South Carolina State House; Cherish Life, n.d.; Nebraska Family Alliance, n.d.
Supreme Court of the United States, 2020 [APPENDIX A Affidavit of Dr. Priscilla K. Coleman]; Shuping and Shaler, ibid; Arizona Supreme Court, n.d.
See, e.g., UK House of Parliament, n.d.; Abortion Grief Australia, n.d.; Society for the Protection of Unborn Children, n.d.; Hope After Abortion, n.d.; Abortion Risks, n.d.; Thorp, 2012: Thorp doesn’t discuss Reardon and Cougle (2002) in-depth, nor seems to be very critical of abortion, but cites Coleman (2011) as a study of importance due to the variance value.
See, e.g., Hope After Abortion, ibid; Abortion Risks, ibid; National Right to Life News, Andrusko (2010): Surprisingly, no mention is made of how Coleman et al. were not consistent on what measurement they used, despite the issue of the measurement being a significant problem; Human Life Alliance, n.d.; Coleman (2010)
For more information, see: Ministry of Truth, 2007; AbyssWriter (2014)
What do you think of this study: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10257365/pdf/cureus-0015-00000038882.pdf ?
"Of 226 women reporting a history of abortion, 33% identified it as wanted, 43% as accepted but inconsistent with their values and preferences, and 24% as unwanted or coerced. Only wanted abortions were associated with positive emotions or mental health gains. All other groups attributed more negative emotions and mental health outcomes to their abortions."